
Time in Range: How CGM Metrics Help You Manage Diabetes Daily
Most people with diabetes know their HbA1c number. It’s the three-month average that doctors use to judge how well your blood sugar is controlled. But what if that number is hiding dangerous spikes and drops you never see? That’s where time in range changes everything.
What Time in Range Really Means
Time in range (TIR) isn’t a fancy term-it’s simple: it’s the percentage of time your blood glucose stays between 70 and 180 mg/dL (3.9-10.0 mmol/L). That’s your sweet spot. If you’re using a continuous glucose monitor (CGM), your device tracks your glucose every 1 to 5 minutes, day and night. Over 14 days, that’s over 1,300 readings. TIR takes all those numbers and tells you how much time you spent in that healthy zone.
The goal? At least 70% of the day. That means 17 hours out of 24 where your sugar stays steady-not too high, not too low. This isn’t a guess. It’s backed by the 2019 International Consensus and the 2025 American Diabetes Association (ADA) Standards of Care. And it’s not just for people on insulin anymore. The ADA now says CGM and TIR should be considered for any adult with type 2 diabetes on glucose-lowering meds, even if they’re not injecting insulin.
Why TIR Beats HbA1c Alone
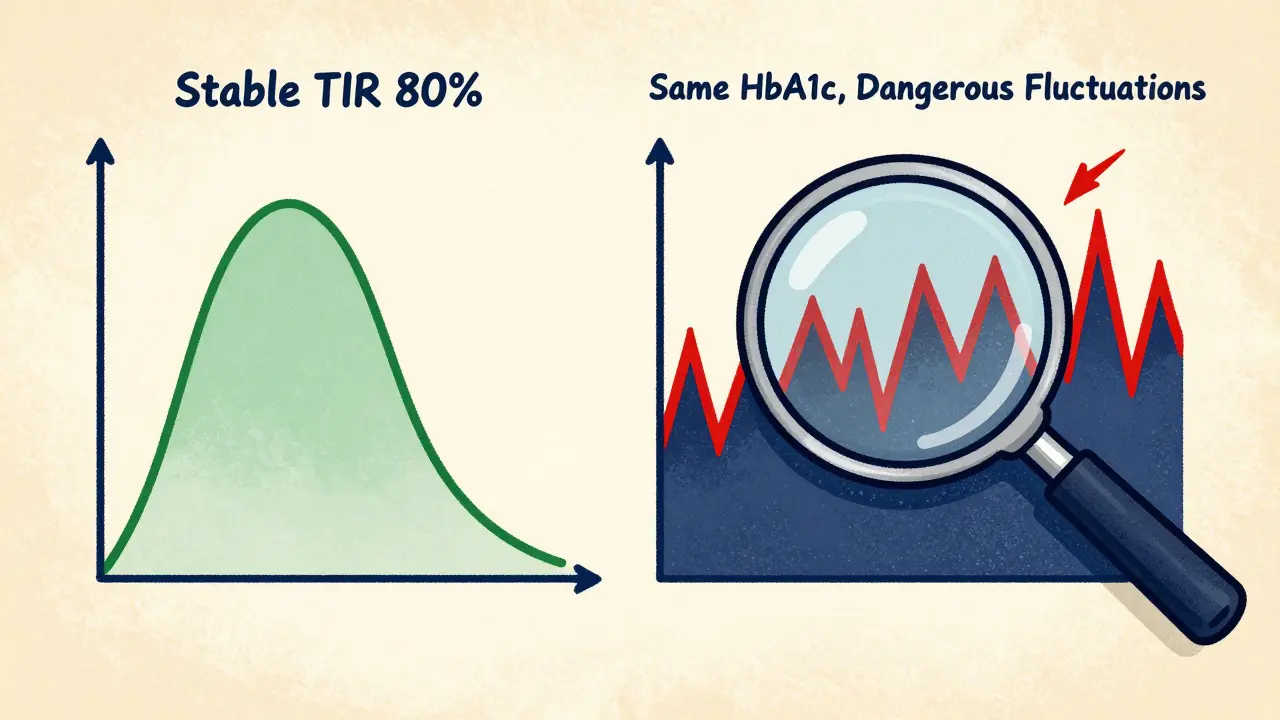
HbA1c gives you a blur. Imagine reading only the last page of a novel. You know how it ends, but you miss all the drama in between. That’s HbA1c. Two people can have the same HbA1c of 7.0%, but one spends 80% of the day in range while the other spends 40% of the day above 200 mg/dL and 10% below 70 mg/dL. One is stable. The other is in danger-facing more risk of nerve damage, eye problems, and dangerous lows.
TIR shows you the full story. It tells you when your sugar spikes after lunch. It shows you if your overnight lows happen every Tuesday. It reveals hidden patterns HbA1c never could. That’s why experts now call TIR a new gold standard-not to replace HbA1c, but to work with it. Think of HbA1c as your yearly report card. TIR is your daily progress log.
The Numbers Behind the Screen
CGM devices don’t just show you one number. They give you a full dashboard:
- Time in Range (TIR): 70-180 mg/dL (target: ≥70%)
- Time Below Range (TBR): Below 70 mg/dL (target: <4%)
- Time Above Range (TAR): Above 180 mg/dL (target: <25%)
- Severe Hypoglycemia: Below 54 mg/dL (target: <1%)
- Glucose Variability: How much your numbers swing up and down (lower is better)
Some people, especially those aiming for tighter control, look at a tighter range: 70-140 mg/dL. That’s closer to what someone without diabetes experiences. Early research suggests this might reduce long-term risks even further, but it’s still being studied. For now, 70-180 mg/dL is the standard for most adults.
How Real People Use TIR to Change Their Habits
One patient in Birmingham noticed her TIR dropped every Thursday. She couldn’t figure out why-she ate the same meals, exercised the same. Then she checked her CGM data. Every Thursday, she had a small glass of orange juice with breakfast. "It’s just juice," she said. But the graph showed her sugar jumped to 210 mg/dL within 20 minutes. She switched to water with lemon. Within two weeks, her TIR went from 58% to 76%.
Another man found his nighttime lows happened after walking his dog at 9 p.m. He’d always thought evening walks were healthy. But his CGM showed his sugar dropped 40 points after each walk. He started walking at 7 p.m. instead. No more nighttime lows.
TIR doesn’t just tell you your sugar is off. It tells you why. And that’s powerful. You start making decisions based on data, not guesswork. You learn which foods spike you, which workouts lower you, and when your stress hits hardest. It turns diabetes management from a chore into a puzzle you’re actually solving.
What You Need to Get Started
You can’t measure TIR without a CGM. The most common devices-Dexcom, Abbott’s Freestyle Libre, and Medtronic-stick to your arm or belly and send readings to your phone. Most wear for 10 to 14 days before needing replacement. The FDA has cleared these devices, and Medicare and Medicaid now cover them for many people with type 2 diabetes who meet certain criteria.
But here’s the catch: you need to wear it. At least 70% of the time. If you take it off for three days, your data isn’t reliable. And you need to learn how to read it. A single glance at a graph won’t help. You need to understand what the colors mean, how to spot trends, and when to call your care team.
Most clinics now offer 1-2 sessions with a diabetes educator to walk you through your first CGM report. They’ll show you how to spot patterns, adjust meals, and respond to alerts. Don’t skip this. It’s the difference between seeing data and using it.

Barriers and What’s Changing
Cost used to be the biggest roadblock. CGMs were expensive, and insurance often only covered them for insulin users. That’s shifting fast. The 2025 ADA guidelines changed everything. By recommending CGM for all adults with type 2 diabetes on glucose-lowering meds-even metformin or GLP-1s-the barrier is falling.
The global CGM market is growing fast. It was worth $4.8 billion in 2022 and could hit $18.6 billion by 2030. More people are using them. In the U.S., CGM use among Medicare beneficiaries with type 2 diabetes jumped from 15% in 2019 to 42% in 2023. More coverage, more data, more proof it works.
Still, some struggle with sensor discomfort, occasional calibration, or just the overwhelm of too much information. That’s normal. You don’t need to fix everything at once. Start by focusing on one thing: your morning spike. Or your after-dinner dip. Tackle one pattern. Then move to the next.
The Future Is Here
AI is starting to help. Some newer CGM apps now suggest small changes: "Try eating protein before carbs," or "Your sugar drops after evening walks-move your walk to earlier." These aren’t magic. They’re patterns you’ve already created, just analyzed faster.
Long-term studies are now linking higher TIR to lower risks of kidney disease, vision loss, and nerve damage. We’re not there yet with absolute proof for every complication, but the trend is clear: the more time you spend in range, the healthier you’ll be.
TIR isn’t just another metric. It’s a shift in how we think about diabetes. It moves us from waiting for a lab result to acting on real-time feedback. It gives you control-not just over your sugar, but over your life.
What’s a good Time in Range percentage?
For most adults with type 1 or type 2 diabetes, aim for at least 70% of the day (about 17 hours) within the 70-180 mg/dL range. This aligns with the ADA’s 2025 guidelines and corresponds to an HbA1c target of around 7%. Some people may aim higher, especially if they’re using insulin or have fewer hypoglycemia risks. Always discuss your personal target with your care team.
Can I use TIR if I don’t take insulin?
Yes. The 2025 ADA Standards of Care now recommend CGM and TIR monitoring for all adults with type 2 diabetes who are on glucose-lowering medications-even if they’re only taking metformin, SGLT2 inhibitors, or GLP-1 receptor agonists. You don’t need to be on insulin to benefit from seeing your glucose patterns in real time.
How long do I need to wear a CGM to get useful TIR data?
You need at least 14 days of wear, with at least 70% of the time actively recording data (meaning no long gaps where the sensor is off or disconnected). Shorter periods can give you a snapshot, but 14 days is the minimum recommended by the International Consensus to capture daily patterns, including weekends and different meals.
Is Time in Range better than HbA1c?
Not better-complementary. HbA1c gives you the big-picture average over three months. TIR shows you the daily highs and lows that HbA1c hides. Two people can have the same HbA1c but wildly different TIR values. TIR helps you adjust your habits today, while HbA1c tells you if those changes worked over time. Use both.
What if my CGM shows I’m in range 80% of the time but my HbA1c is still 8.0%?
This can happen, and it’s not unusual. HbA1c reflects average glucose over time, but it’s also influenced by how long your sugars stay high versus how often they dip low. If you have frequent low glucose events-even brief ones-they can lower your HbA1c even if you spend a lot of time high. Your care team may look at your Time Above Range (TAR) and glucose variability to understand the full picture. You might need to reduce high spikes even if your lows are under control.
Time in range isn’t about perfection. It’s about progress. One extra hour in range today is one less spike tomorrow. And that’s how diabetes care is changing-for the better.





8 Comments
phyllis bourassa
March 8 2026Okay but let’s be real - if your TIR is below 70%, you’re basically playing Russian roulette with your kidneys. I’ve seen people brag about their HbA1c being ‘perfect’ while their CGM shows them spiking to 280 after toast. Bro. No. Just no. Your body isn’t a spreadsheet. It’s a fragile, beautiful machine that deserves better than ‘close enough.’
And don’t get me started on those ‘I don’t need CGM’ folks. You’re not saving money - you’re just delaying the amputation.
Also, why is no one talking about how much mental energy this takes? Constant monitoring. Constant guilt. Constant recalculating. I love my CGM, but it’s also my emotional vampire.
amber carrillo
March 8 2026Time in range is a game changer. It turns abstract numbers into actionable insight.
For years I focused on HbA1c alone. Then I got a CGM. The difference was like going from black-and-white TV to HD.
Now I know when my coffee spikes me. When my stress drops me. When my sleep affects me.
This isn’t just data. It’s self-knowledge.
Tim Hnatko
March 9 2026I’ve been using CGM for 18 months now. I didn’t think I needed it - type 2, not on insulin, felt fine.
Turns out I was having silent lows. Like, 5:30 a.m. every day. No symptoms. Just fatigue. I thought it was aging.
Once I saw the pattern, I adjusted my dinner. Now I’m at 82% TIR. No more 3 p.m. naps. My wife noticed. She said I ‘stopped being a zombie.’
Small changes. Big difference.
Aaron Pace
March 11 2026OMG YES 😭
I used to think HbA1c was the whole story. Then I saw my CGM graph after a weekend of ‘cheat meals.’
It looked like a rollercoaster made by a toddler.
Now I eat like a monk. And I’m not even mad about it. 🥹
My TIR went from 58% to 84% in 3 months. I feel like a new person.
Also I named my CGM ‘Bobby.’ He’s my best friend now.
Joey Pearson
March 12 2026If you’re not using TIR, you’re flying blind.
Stop waiting for your doctor to tell you. Get a CGM. Track it. Adjust it.
Your future self will thank you.
And yes - even if you’re not on insulin. Yes - even if you think you’re fine.
You’re not.
Roland Silber
March 13 2026There’s a quiet revolution happening in diabetes care, and TIR is at the center of it.
The shift from HbA1c as the sole metric to TIR as the daily guide is one of the most important clinical advances in a decade.
It’s not about perfection. It’s about pattern recognition.
What matters isn’t just whether you’re in range - it’s why you’re not in range.
That’s where real learning begins.
And yes - the ADA recommendation for all type 2s on glucose-lowering meds? Long overdue.
It’s not about insulin. It’s about insight.
Patrick Jackson
March 15 2026I used to think my diabetes was ‘under control’ because my HbA1c was 6.8.
Then I saw my CGM data for the first time.
It was like watching a horror movie where I was both the victim and the villain.
Every spike. Every crash. Every silent night of 60 mg/dL.
I cried.
Not because I was scared.
But because I finally saw the truth.
It wasn’t that I was failing.
It was that I was blind.
Now I don’t just manage diabetes.
I listen to it.
And it talks back.
Adebayo Muhammad
March 17 2026Let me be perfectly clear: the entire paradigm of diabetes management is built upon a flawed statistical abstraction - HbA1c - which, by its very nature, is a grossly aggregated, temporally obfuscated, and statistically misleading metric that fails to capture the dynamic, non-linear, and highly individualized physiological reality of glucose homeostasis.
Moreover, the promotion of TIR as a ‘gold standard’ is not a scientific advancement - it is a commercialization of surveillance capitalism disguised as patient empowerment.
Who benefits? The CGM manufacturers. The data brokers. The algorithmic health-industrial complex.
And who pays? The patient - in time, anxiety, and financial burden.
Do not mistake visibility for healing.
Do not mistake data for wisdom.
Do not mistake surveillance for care.